
Ankle arthroscopy is also known as key hole ankle surgery (or minimally invasive ankle surgery). It is an operation performed under general or regional anaesthetic and involves using two very small incisions to gain access into the ankle joint. Each incision is less than 1cm and usually two incisions are required both to give different perspectives of the joint as well as to allow the insertion of special instruments from the opposite side to that for the camera.
The ankle joint is relatively small and to allow good surgical access to the joint, its dimensions need temporarily to be increased. This is done using a combination of traction across the joint together with a flow of pressurised fluid circulating through the joint which distends it.
Not all ankle surgery can be done using arthroscopy but there are certain conditions for which it is commonly used. These include ankle arthritis , ankle impingement ,ankle instability ,pain following ankle fracture ,osteochondral defects ,loose bodies and synnovitis.
The alternative to arthroscopy is open ankle surgery which results in larger scars and generally somewhat more post-operative pain. For certain cases though this is unavoidable.
The very small incisions required for ankle arthroscopy result in minimal soft tissue disruption and trauma. This in turn means:
- Significantly lower pain levels than with an open approach
- The ankle is comfortable to weight bear through on the day of surgery
- Most cases can be performed on a day case basis
- Lower infection rates than opting for the open surgical approach
- Earlier return to work/function/sports
- Little scarring
- Minimal effect if further surgery to the ankle is required
The ankle joint has small internal dimensions under normal circumstances. To produce sufficient space in which to perform the ankle arthroscopy procedure and avoid damaging the joint surfaces with instruments, it is necessary to “stretch open” the joint. This is achieved under anaesthesia by using a combination of traction across the joint and distending the joint by infusing sterile fluid under pressure.
Most ankle arthroscopy is performed under general, or occasionally regional, anaesthesia. Firstly when setting up the patient a padded bar is placed behind the thigh as shown.

Next a strap is placed around the ankle and connected to a second bar distant from the first which is attached to the operating table and allows traction to be placed across the ankle. In this way the ankle is stretched open sufficiently to allow a space with sufficient dimensions in which to operate.

Sterile fluid is infused under pressure into the ankle joint through the camera system (1) whilst the shaver or other instruments are inserted through a separate portal (2).

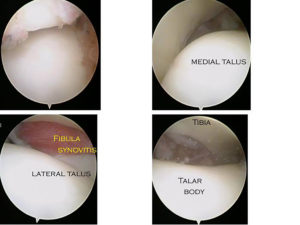
It should be possible to see the majority of the joint surfaces of the Talus , distal Tibia and Fibula during ankle arthroscopy. The lining of the joint when healthy should be white , smooth and without any evidence of irregularity or breach(as in all these images). Inflammation of the joint lining (synnovium) can occur for many reasons and is abnormal and often produces symptoms. Such an area of synovitis is seen here located next to the Fibula. There are wide gaps between the Talus ,Tibia and Fibula due to the fact these images are taken during an ankle arthroscopy when the joint has been distracted (stretched open).
The unstable ankle: An ankle may become unstable because its ligaments have been injured and are no longer competent . This is known as mechanical instability and though ankle arthroscopy will not by itself treat this condition, there are often associated problems within the ankle joint which will require an arthroscopy. In addition it may also be necessary to address the ligaments by reconstructing them.
An ankle may also be functionally unstable. This is when the normal mechanical restraints ( tendons and ligaments) are working fine, but the ankle nevertheless feels unstable. This is usually due to a painful area within the joint such as a synovitis (inflammed tissue in the joint), a plica or arthrofibrosis(scar tissue in the joint) or a chondral or osteochondral injury (damage to the bone & cartilage lining of the joint). All of these conditions can be treated using an ankle arthroscopy.

Anterior ankle synovitis before and after removal with an arthroscopic shaver
Ankle pain following a fracture or sprain :Following an ankle fracture which has healed, there are a number of causes for ongoing pain. If the joint surface has been disrupted and either portions of the joint have been lost or it has not been possible to restore the joint back to its normal dimensions then arthritis may ensue with the symptoms that brings. Occasionally, the metalwork used to fix an ankle fracture can become prominent or seem to be tender superficially and this would also produce pain. Very rarely, a condition known as a regional pain syndrome may occur, which will produce ongoing pain following ankle fracture. Generally, any residual symptoms after an ankle fracture stand a chance of improving for twelve to eighteen months following the injury, depending on the underlying diagnosis. If symptoms persist and the preceding conditions have been excluded then there may be problems within the joint itself which are leading to ongoing symptoms. Common findings are either chondral or osteochondral injury, synovitic lesions, loose bodies or post-traumatic fibrosis.
Footballers Ankle :This is a condition which is most often present in those who have engaged actively in sports for a number of years. Footballers ankle manifests itself with pain at the front part of the ankle joint which remains well localised and occurs mainly during dorsiflexion of the ankle( when the foot moves towards the shin ). It is due to spurs of bone forming usually on the front of the Tibia at the ankle joint. A spur of bone at the front of the ankle is also a common finding in ankle arthritis. In ankle arthritis the joint surfaces are not normal and pain is less specific and more consistent .Usually in a footballers ankle the joint surfaces are normal.
Ankle osteoarthritis :Debridement or fusion are the two arthroscopic options for an osteoarthritic ankle. See ankle arthritis section for detail on this. Ankle arthroscopy can be usefully used to debride (tidy up) mild or moderately arthritic joints.
. 
Loose bodies :Loose bodies are pieces of bone and cartilage which either float freely between a joint or sit loosely attached at the margin of the joint. If these jar between the surfaces of the joint they may cause symptoms of instability or pain. This tends to be intermittent rather than continual. They can also produce symptoms of instability.
Diseases of the synovium :The synovial joint lining itself may become diseased as the primary complaint within the ankle joint. Conditions which cause this are diseases such as rheumatoid arthritis or synovial chondromatosis. The symptoms are those of pain or instability and arthroscopy again can assist. In both these cases the conditions however have a tendency to recur . 
Synnovial chondromatosis(1)

Obviously determined by the conditions treated & associated procedures
Assuming a straight-forward soft tissue arthroscopy then reduce the compressive ankle bandage at 5 days and patient may drive from then.
Wounds to be kept strictly covered by breathable dressings 24/7 and dry until 2 weeks.
Sutures removed at this stage . It is fairly usual to need to steri-strip one or other portal and keep covered another 5-7 days due to slow wound healing in this area. Earlier wound exposure risks superficial infection which can progress to deep infection with rapid speed. Any simple arthroscopic portal erythema should be aggressively treated with high dose oral antibiotics and very early clinical review.
Numbness associated with superficial nerves is not uncommon despite taking measures to minimise its occurrence. It is not unusual for this to occur as the surgical scars thicken during the first 6-8 weeks post-operatively. A desensitisation routine should be aggressively instigated.
Beyond 2-3 weeks patients may shower the ankle .
The first two weeks post-op the patient should aim simply to return to comfortable walking.
Once this is achieved they may start physio rehab and during week 3 work on gentle strengthening and balance , using a static bike for exercise. Week 4 & 5 are spent using cross-trainer and week 6 light jogging.
The realistic expectation after ankle arthroscopy for removal of soft tissue pathology is for largely unrestricted activity by 6 weeks.
If the indication for operation has been early ankle arthritis (where arthroscopy in my opinion has a significant role ) then the time by which a steady state is likely to have been reached is on average 12 weeks and not 6. There is also an associated risk of immediate deterioration , maybe in 5% of patients , necessitating further operative treatment (most commonly fusion or replacement).
Septic arthritis presents with increasing pain , decreased ability to weight bear and move the joint and septic symptoms (unless the patient is immuno-compromised in which case symptoms early on my be minimal). Any suspicion of the diagnosis mandates as a minimum a joint aspiration in sterile surroundings (through non-inflammed skin) and an immediate gram stain as well as appropriate analgesia and joint splintage and IV “best-guess’ antibiotics. Immediate thorough operative joint lavage and commencement of best guess high dose IV anti-staphlococcal antibiotics is required after baseline inflammatory markers have been taken.
Ankle Arthroscopy for ankle arthritis
I first consulted Mark Herron in 2006 after experiencing severe pain and limited mobility with my right ankle. Mark went through all the options for me and decided an ankle arthroscopy would give me the best long term solution. At best it would hopefully improve symptoms for about 4 years. I am pleased to say Marks expertise far exceeded this and my symptoms did not become problematic for 10 years. I am now back in Marks care and I have every confidence he will once again restore me back to good mobility. Thank you to everyone on his team.
H Driver – Birmingham 2017
Ankle Arthroscopy for post injury pain
Having suffered for 18 months with a sport related injury, I was referred to the Foot and Ankle Clinic in Birmingham by my GP.
My initial appointment through to surgery was extremely quick. The staff were exceptionally knowledgeable and made me feel very confident about the whole procedure.
The facilities at the Foot and Ankle Clinic were first class and the team of staff were professional and welcoming. The result of my treatment has been fantastic, going from a very painful and swollen ankle with limited mobility to pain free with almost 100% mobility. I cannot believe I didn’t visit the Foot and Ankle Clinic earlier.
The surgery has made a massive difference to my quality of life.
Mr P Geddes
West Midlands
Ankle Arthroscopy for Osteochondral defect of Talus
I was referred to the Foot and Ankle clinic by my physiotherapist in late 2008 after suffering ligament damage to my ankle playing football. After a prompt MRI scan I was scheduled for an ankle arthroscopy during which further cartilage damage were discovered. This problem was dealt with by way of microfracture surgery and after a 6 week non-weight bearing period I am back to full fitness. I would recommend the Foot and Ankle Clinic on the basis of the speed with which the whole process was dealt with together with the extensive specialist foot and ankle expertise.
Mr J Catling
Birmingham
Ankle Arthroscopy for Osteochondral Defect of Talus
In July 2006 I fell off my horse and broke the talus bone in my foot. After 16 months I was still suffering with discomfort in the foot, I had very poor walking gait and my muscles were very tight and tired easily. I decided to get a second opinion and was recommended to the Foot and Ankle Clinic.
I was seen very promptly an xray and MRI scan were all done on the same day. The scan revealed I had a piece of loose bone at the top of the talus and a build up of scar tissue. This meant a small operation using keyhole surgery needed to be performed, a date was fixed at my convenience.
The operation was performed and all went well. Only a few hours after the operation I could already feel the difference. The foot was immediately more mobile. I then had 6 weeks of non-weight bearing, after that I was able to start rehabilitation. After 6 months my foot is back to normal. It was such a relief to regain full use of my foot, I am very grateful for all the care I have received at the Clinic.
E J Edge
Worcestershire
Ankle Arthroscopy for post traumatic pain
I received 1st class surgery and treatment to my left ankle at the Foot and Ankle Clinic. With much improved range in my ankle I experienced less pain and a tidy scar.
I would recommend the Foot and Ankle Clinic to anyone and definitely would return.
T Edwards
Sutton Coldfield
Ankle Arthroscopy for ankle arthritis
“There is no doubt that it is a lot better but I am not completely pain free. Last year it was painful to walk about at work and mowing the lawn was an ordeal. I don’t notice it doing these activities now. I have stopped running. I did try running on it for about a mile but it was painful and swollen afterwards and I realised this was not going to be a good idea…….. Cycling is no problem and walking is much better. I can manage at least a 4 hour mountain walk without problems. … In summary, I am pleased with the work you have done. I don’t think I am ready for arthrodesis just yet. ….”
Dr N Brown ,Birmingham
Subtalar Arthroscopy
I was first referred to the Foot and Ankle Clinic by my physiotherapist after non-operative intervention. The reputation of the Clinic was a priority to me and I heard from more than one source that it is one of the best in the field. My surgery was a complete success and I would recommend to anyone requring similar treatment.
Mr A Liddiard
Birmingham