

The current generation of ankle replacements are prostheses which resurface the two main bones articulating at the ankle which are the tibia (shown above) and the Talus (shown below).
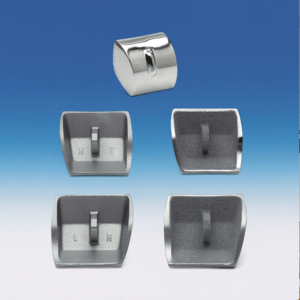
In other words they “reline” the joint, by replacing the worn out joint surfaces. These components are made of metal.
Between the two components sits a plastic (UHMWPE) spacer, the meniscus (shown below)

The meniscus allows movement on both its upper & lower surfaces. The addition of this component, though not present in the normal ankle, allows the artificial joints movement to match the normal ankle more closely and in particular rotate as well as flex and extend.
This ability to match the normal ankles movement also significantly improves the durability of the joint (compared to the first generation of ankle replacements which were designed as directly linked hinges). These early replacements failed rapidly by forcing the normal rotation of the human ankle to occur at the interface of the bone and implant , given the mechanical hinge joint implanted did not allow for this.
The illustrative diagrams are of the STAR ankle replacement, which is one ankle replacement we use at the Clinic. This has been in use for over 20 years, in various forms. An equally tried and tested prosthesis is the Buechel-Pappas. There are also other newer prostheses available, though these have the disadvantage of relatively limited evidence as to their longevity, one of the main factors to consider before implantation.
An ankle replacement works by removing the worn out joint surfaces which are generating the pain and as a result the ankle pain disappears in most (but not all) patients. Replacing them with a mobile weight bearing surface means that existing ankle movement can be retained. Adequate muscle and tendon function is also required for a successful outcome so it is an implant best avoided if there is neurological compromise.
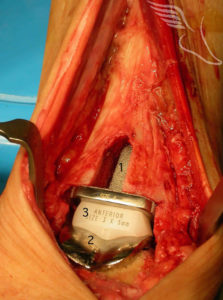
Both components have bioactive coatings which encourage the growth of bone onto them, forming a natural bond with the implant. This type of implant coating is well illustrated on the tibial stem of the ankle replacement shown here.
This is a procedure whose indication is chronic severe arthritic pain (as with other joint replacements).
How much pain and for how long is a personal choice and fairly subjective but it is an operation for severe ankle arthritis.
Its main advantage over ankle fusion is that it maintains the movement at the ankle joint whereas after a fusion movement into flexion and extension is from the subtalar and midfoot joints. As long as these are healthy and non-arthritic then a long period of high level function can be expected after a successful ankle fusion. If these joints are already arthritic then a replacement is one option that should be considered. In the longer term after an ankle fusion it is likely that the subtalar and midfoot joints will become arthritic as a result. This is likely to not be before 15 years + and is unlikely to require subsequent surgery however. Such a situation is illustrated by the X-Rays below.


Generally patients for an ankle replacement should be over the age of fifty. This relates to probable higher functional requirements in the younger age group and as a result likely reduced longevity of the joint. The age of fifty is not an absolute lower limit. An exception to this would be a younger patient with multiple arthritic joints (such as with severe rheumatoid disease) who is likely to have low functional requirements and may have rapid progression of arthritis in the joints compensating for the ankle if it were to be fused.
As important as age are the functional requirements of any patient. Those in ‘heavy manual’ occupations (builders, farmers, heavy industry workers) who are over fifty are probably better advised to undergo an ankle fusion especially if they have isolated ankle arthritis. Accelerated wear is likely if the joint has heavy usage.

The first 24 hours
Pain relief
This is by means of a regional femoral and sciatic nerve blockade supplemented by tablets or PCA .
Cast/splintage
A temporary plaster cast will be applied after the operation and changed the next day to a light weight cast or removable Thermoplastic splint.
Oxygen therapy
To reduce the chance of wound complications (breakdown /slow healing) we routinely advocate supplemental oxygen (via nasal prongs) for 24 hours.
DVT prophylaxis
Clexane for 6 weeks unless contraindicated.
Length of stay
You will require on average two days post operatively in hospital.
Physiotherapy
Within 24-48 hours you will be mobilised non weight bearing. This means using two crutches for walking .
Generally this continues for 4-6 weeks after the operation date.
At two weeks
Outpatient visit to ensure wounds have healed and a change of cast .
At six weeks
Weight bearing out of cast commenced, with physiotherapy, following a check x-ray and outpatient visit.
At three months
Return to driving.
Long term annual follow up required.
1% Deep infection (of the joint)
1% Wound infection
5% Delayed wound healing/breakdown
1% DVT/PE
3%-5% Pain and stiffness despite replacement.
10% Malleolar(ankle) fracture
Failure of implant (85% 10 year survivorship approximately)
My ankle replacement came after experiencing tremendous pain in my ankle due to arthritis which badly affected my quality of life.
After the ankle replacement surgery I am now back to full, pain-free mobility – no limp! My return to my hobby of shooting, walking working dogs all day for 3 to 4 days a week over many uneven ploughed fields, slopes and woodland was achieved without any discomfort.
I can thoroughly recommend an ankle replacement – it gave me back a pain free perfect ankle and my quality of life – even at 70+ years of age.
R Kendrick
Worcestershire
In March 2007 I had an ankle replacement operation at the BMI Priory Hospital in Birmingham.
The expertise of the surgeon and the nursing staff resulted in a very successful operation. The very high standard of hygiene and after care of all the staff gave me great confidence.
The Pre-operative information I received was of great value to me and I would have no hesitation in recommending the Foot and Ankle Clinic to any future patient.
After a year, my mobility and freedom from pain is amazing and I am very thankful I underwent the operation.
G Rollason
Shropshire
One of the best things I did was find someone who’d already had an ankle replacement and spending an afternoon talking to her. It was then that I definitiely decided to proceed with the surgery.
There were two days in the hospital with the operated leg being surprisingly free from pain given the circumstances.
Some eighteen months after the ankle replacement operation I would say that I am a very satisfied customer with a full range of movement, just the same as the other side and walking normally without pain.
E Coward
Birmingham